Supraspinatus: optimal mechanics. Tendonitis of the supraspinatus muscle of the shoulder joint treatment
Due to certain functional and anatomical features, damage to the supraspinatus muscle of the shoulder develops in almost half of all cases of injury. Timely diagnosis and adequate treatment allow maintaining the functional state of the shoulder, as well as reducing the duration of the rehabilitation period.
Structural features
The shoulder joint has a round shape, which allows the movement of the upper limb in 3 different planes. This form requires additional stabilization to prevent dislocation. Certain structures provide strength and stability, which is why they are called the anatomical cuff. These include the rotational (rotator), subscapular, infraspinatus and supraspinatus muscles of the shoulder. Damage to the tendon (they are strong fibers attached to the bone base) occurs under certain conditions, accompanied by a significant impact of force. This often develops a simultaneous violation of the integrity of one or more components of the anatomical cuff.
Pathogenesis
The pathogenesis of the development of changes in the structures of the musculoskeletal system, including the cuff, consists in the implementation of 2 mechanisms:
- Significant force acting on the shoulder, as a result of which pressure is exerted on the structures of the cuff by the head of the humerus.
- Decrease in the strength of the fibers of the structures, which primarily affects the tendon. In this case, damage can develop against the background of normal loads.
Elucidation of the mechanism of development, due to the implementation of which damage to the supraspinatus muscle of the shoulder joint occurs, makes it possible to select the most effective therapeutic tactics in the future.
Provoking factors
A significant effect of force on the shoulder can be in various situations, which include falls on an outstretched arm, excessive extension, and blows. The decrease in the strength of the fibers is the result of the development of pathological processes:
- Degenerative-dystrophic pathology, which is the result of malnutrition of cartilage structures with their subsequent destruction.
- Inflammatory conditions - tissue damage is due to the development of an infectious, autoimmune (the appearance of antibodies to one's own tissues that damage the structures of the musculoskeletal system) process.
- Congenital change in the properties of the connective tissue structures of the body, which has a genetic hereditary origin.
Elucidation of the main cause that led to changes in the structures, in particular the supraspinatus muscle, is necessary for the choice of preventive measures in the future.
Classification
 Injury to the tendon of the supraspinatus muscle of the shoulder joint is classified according to several criteria that are clarified during the diagnostic process. Depending on the degree of change, there are:
Injury to the tendon of the supraspinatus muscle of the shoulder joint is classified according to several criteria that are clarified during the diagnostic process. Depending on the degree of change, there are:
- Partial supraspinatus tendon injury is a milder form of trauma in which the overall structure and shape is preserved. There is a rupture of individual fibers, the total length of the tendon increases, so this damage is also called sprain or intratendinous damage to the tendon of the supraspinatus muscle.
- A complete rupture of the tendon is usually in the region of the lesser tubercle of the humerus, which is accompanied by a violation of the form and function.
- Combined changes in which the joint capsule is affected.
According to the main mechanism of changes and the group of provoking causal factors (pathogenetic and etiological criteria), 2 forms of changes are distinguished:
- Degenerative damage to the tendon of the supraspinatus muscle of the shoulder is a violation of integrity, which in most cases is the result of malnutrition of connective tissue structures.
- inflammatory changes.
- Post-traumatic violation of the integrity, occurring against the background of unchanged structures.
There are also 3 degrees of severity of the pathological condition. The division of changes in the structures of the cuff allows the orthopedist-traumatologist to choose the optimal therapeutic tactics and subsequent rehabilitation.
Symptoms
The clinical picture of changes includes several rather characteristic manifestations:
- Pain in the shoulder area, the intensity of which depends on the severity of the changes. After an injury, the pain is acute, in the case of the development of a pathological process (inflammation and degenerative-dystrophic process), it develops and intensifies gradually.
- Limitation of active movements - it is difficult for the patient to withdraw the arm, this is especially noticeable when the arm is abducted by 60 °.
- The appearance of signs of an inflammatory reaction, which include reddening of tissues due to increased blood flow, swelling with the release of the liquid part of the blood into the intercellular substance, as well as pain associated with direct irritation of sensitive nerve endings.
The appearance of several signs of changes in the integrity of the structures of the cuff significantly reduces the quality of life of a person and is the basis for contacting the appropriate medical specialist.
Diagnostics
Most changes in the structures of the musculoskeletal system are accompanied by similar clinical symptoms. Therefore, a reliable clarification of the etiology, the degree of changes is performed using diagnostic techniques.
Modern research methods include visualization of the structures of the musculoskeletal system using radiography or fluoroscopy, endoscopic techniques (arthroscopy), tomography (methods with a high separation power of imaging), ultrasound examination. To determine the cause of the disease, as well as to determine the severity of functional changes, laboratory tests are prescribed.
Treatment
 Usually, medical specialists, regardless of the cause and nature of the changes, prescribe a radical treatment, including surgical manipulations. In specialized clinics, arthroscopic surgery is predominantly performed, because its implementation is accompanied by minimal tissue damage (a special tube with a light source, a camera and micromanipulators is inserted to access the internal structures).
Usually, medical specialists, regardless of the cause and nature of the changes, prescribe a radical treatment, including surgical manipulations. In specialized clinics, arthroscopic surgery is predominantly performed, because its implementation is accompanied by minimal tissue damage (a special tube with a light source, a camera and micromanipulators is inserted to access the internal structures).
In case of incomplete rupture, conservative treatment with the use of NSAIDs, chondroprotectors, vitamins, physiotherapy (ultraphonophoresis with drugs, magnetotherapy) can be prescribed. Increasingly, as part of a conservative tactic, the introduction of platelets into the joint, which contain substances that stimulate tissue repair, is being used.
Rehabilitation
The final restoration of shoulder function is possible during rehabilitation. It includes special exercises in which there is a gradual adaptation of the structures to the loads. The duration of events varies from several months to six months.

Shoulder pain is a problem that regularly worries thousands of people all over the planet. There can be several reasons for discomfort in the shoulder and arm area, one of them is supraspinatus tendinitis. The supraspinatus muscle abducts the arm to the side, and its inflammation makes training unbearable.
Tendinitis is an inflammatory disease that affects the tendons. Pathology provokes pain and can cause serious complications, which is why doctors recommend contacting a specialist at the first sign of tendonitis. Timely treatment will help improve the quality of life and prevent the transition of the disease into a chronic form.
Supraspinatus tendonitis
Tendinitis of the tendon of the supraspinatus muscle of the shoulder is a disease of athletes, as pathology occurs with constant and heavy loads. But in medicine, there are also cases of tendinitis of the supraspinatus muscle in people who practically do not play sports, and this is understandable.
Typically, such a patient leads a passive lifestyle, does not exercise, and as a result, has weak muscles. One day, he suddenly decides to go in for sports, for his health, or for fun, but he does not take into account his physical condition. Excessive stress can lead to tendon injury and inflammation.
The following conditions can also provoke tendinitis of the supraspinatus muscle of the shoulder joint:
- trauma;
- excessive physical activity;
- monotonous hard work;
- rheumatism;
- local infections.
Tendinitis of the supraspinatus and subscapularis muscles
Tendinitis of the supraspinatus muscle of the shoulder, in the absence of timely treatment, can pass to the subscapularis muscle, which worsens the patient's condition. This usually happens if the patient ignores the pain, does not go to the doctor, and continues to systematically load the sore shoulder.
Tendonitis of the supraspinatus and subscapularis muscles is accompanied by the following symptoms:
- pain that occurs during physical exertion, at rest, it may not be felt at all;
- in the area of \u200b\u200bthe tendons of the affected muscles, edema is observed;
- with active movements, a crunch is heard;
- on palpation of the inflamed muscle, pain is felt.
If the cause of inflammation is an infection, then the symptoms are more pronounced. The affected muscle is red, hot, painful. The general condition of the patient is poor, he is worried about weakness and high temperature. This condition can be very life-threatening if the infection causes sepsis.
Calcific supraspinatus tendonitis
Calcifying tendonitis of the supraspinatus tendon is a type of disease in which calcifications are deposited in the area of the tendon and muscle, with further inflammation. Calcific tendinitis can be reactive and degenerative.
Degenerative is associated with increased stress on the joint, tendon wear, tissue malnutrition. In this case, micro-tears occur in the tendon, which do not have time to heal, and calcium is deposited in them. The exact cause of reactive calcification has not been established, but it is known that with this form of the disease, calcifications can resolve on their own.
Treatment of supraspinatus tendinitis
Tendinitis of the tendon of the supraspinatus muscle of the shoulder joint requires mandatory and timely treatment. If the patient ignores pain during training and continues to load the sore shoulder, the disease will soon become chronic.
Chronic tendinitis of the tendon of the supraspinatus muscle is difficult to cure, the pathology will disturb with constant relapses and make any load unbearable.
Diagnosing supraspinatus tendinitis is usually not difficult, it is enough for a doctor to conduct an external examination and listen to the patient's complaints in order to make a correct diagnosis. In severe cases and in the presence of calcifications, ultrasound may be needed.
With a timely visit to the doctor, tendinitis of the shoulder is treated conservatively. First of all, the doctor forbids loading the sore shoulder, training for the duration of treatment must be completely stopped. Wearing an orthosis or an elastic bandage may be recommended to fix the shoulder.
Non-hormonal anti-inflammatory drugs are prescribed to relieve pain and inflammation. They are used in the form of tablets and externally in the form of ointments and gels, examples of such agents include Ibuprofen, Nimesulide, Diclofenac. These remedies reduce pain and relieve inflammation in the affected muscle. In more severe cases, hormonal agents are prescribed, for example, Cortisone.
Also, patients are shown physiotherapy, for example, electrophoresis, magnetotherapy, special physiotherapy exercises and professional massage. All procedures are prescribed individually for each patient, depending on the stage of the disease.
If conservative treatment fails, or supraspinatus tendinitis is advanced, surgical treatment may be recommended. The doctor will remove calcifications using arthroscopy, which will speed up recovery.
Source: http://sustavof.ru/tendinit/tendinit-nadostnoj-myshtsy.html
Tendinitis of the shoulder joint - diagnosis and prerequisites for occurrence!
The shoulder joint is one of the large movable joints of the bones in the human body. He is able to perform a variety of movements. Therefore, the pain that appears in it can greatly affect the quality of human life. One of the most common causes of pain in the shoulder joint is tendonitis.
Shoulder tendonitis
What is shoulder tendinitis?
Tendinitis of the shoulder joint is an inflammation of the tendons of this mobile joint of the bones. About 2% of people experience this disease at least once in their lives.
Inflammation of the tendons - tendinitis
Tendons are dense connective tissue strands designed to connect muscles to the surfaces of bones.
The joint of the shoulder is formed by parts of two bones:
- scapular articular cavity;
- head of the humerus.
Shoulder Anatomy
The areas of the bones facing the joint are covered with cartilage. The head is much larger than the area of the scapular articular surface. Because of this anatomical feature, the tendons of the five muscles that form the muscle capsule are under a lot of stress. This fact explains why pain in the shoulder is often caused by tendinitis.
Especially often, inflammation occurs due to the increased load on the shoulder joint. But there may be other reasons as well.
Origin of shoulder tendonitis
Inflammation and pain in tendonitis
The inflammatory process in the tendons is determined by various factors, but great physical exertion plays a primary role. Intense and prolonged muscle contraction leads to strong tension, small tears and inflammation in the tendon.
Due to heavy physical exertion, tendinitis of the shoulder joint is often found in athletes, painters, gardeners, movers, etc. Age-related loss of elasticity in persons of either sex and hormonal changes in the female body during menopause only increase the risk of tendon inflammation.
A large load on the joint can provoke inflammation
Note! It is because of the connection with endocrine restructuring that tendinitis is more common in women.
Tendonitis in women is not uncommon.
But tendon inflammation has several other causes:
- long-term fixation of the hand due to injury, for example, with long-term use of gypsum;
- articular pathologies, such as psoriatic arthritis or gout;
- weakening of the immune system as a result of taking glucocorticosteroid drugs, chemotherapy, bone marrow transplantation, etc.;
- endocrine disorders (diabetes mellitus and thyroid dysfunction);
- systemic lupus erythematosus and other autoimmune pathologies;
- infections penetrating the inside of the joint and spreading to the strands of the tendons, for example, gonorrhea, boreliosis, streptococcus;
- articular injuries, mainly with their improper treatment;
- osteochondrosis of the neck;
- curvature of the spinal column and violation of posture;
- stressful effects leading to muscle spasm, which increases the intensity of the tendon;
- drug allergy;
- congenital musculoskeletal disorders.
Any of these causes leads to the main manifestation of tendonitis - pain.
Pain and inflammation can occur for various reasons.
Symptoms of the inflammatory process in the tendons of the shoulder
Tendinitis of the shoulder joint is manifested by various symptoms:
- pain syndrome;
- limited movement;
- reddening of the skin, fever and swelling at the site of inflammation.
The first two signs are the main ones.
Soreness and limited movement are the main symptoms
Soreness with inflammation of the tendons has several characteristics.
- It has a shooting or dull, aching character.
- It often torments a person during a night's sleep, which can even lead to insomnia.
- It is localized mainly in the joint area. Rarely, its spread to the elbow can be observed.
- Usually fades and even completely disappears at rest.
The locality of pain sensations and their appearance only during movement are one of the signs that, already at the stage of physical examination, help to make a differential diagnosis of tendinitis and arthritis.
Pain syndrome is the cause of the appearance of the second obligatory symptom - motor limitation. It is difficult for a person to perform simple movements: comb his hair, put his hand back or raise it, etc. At the same time, at the very beginning of the inflammatory process, only active movements are limited due to pain, that is, those carried out by the patient himself.
It hurts to move your arm and your shoulder hurts - there is a reason for an urgent visit to the doctor
Note! Restriction of movement in the absence of therapy often becomes chronic. In advanced cases of the disease, the patient can only raise his arm 90 degrees.
The nature of the change in motor activity depends on the type of tendinitis.
Types of inflammation of the tendon of the shoulder
Tendinitis of the shoulder joint is a collective name. In the practice of an orthopedist and traumatologist, inflammation of the tendons in the area of the scapular-shoulder joint, indicated in the table, is more common.
| calcifying | differs in calcium deposits; in the degenerative form, calcium salts are deposited at the sites of damage to the tendon; the mechanism for the appearance of the reparative type is not fully understood; the maximum pain syndrome is observed during the resorption of calcium deposits; pain intensifies when raising the arm up; tendons of the periosteal muscle are more often affected; complete cure; often recurs. |
| Inflammation of the biceps tendon | It is formed against the background of a heavy load, for example, in tennis players; pain is localized in the upper and anterior zone of the shoulder; leads to difficulty in lifting heavy objects. |
| develops with a traumatic impact on the tendon by the acromion (the edge of the scapula facing the collarbone), the joint formed by the acromion and the clavicle, or the ligament of this joint; leads to difficulty moving the arm away from the body to the side. | |
| Tendonitis of the infraspinatus and teres minor | accompanied by pain when rotating the shoulder back. |
| Inflammatory lesion of the tendon of the subscapularis muscle | Characterized by pain when turning the shoulder inward. |
Inflammation of the tendons of the supraspinatus, infraspinatus, teres minor, and subscapularis muscles is collectively referred to as rotator cuff tendonitis. But the supraspinatus muscle suffers more often.
Tendinitis of the rotator cuff
Tendinitis of the shoulder joint also differs in severity. In total, 3 types are distinguished, which differ in a different clinical picture.
- The pain is aching and not intense. It appears only when moving jerkily. The x-ray image shows no changes.
Intense aching pain
- The sensation of pain intensifies and accompanies any independent physical activity. When fluoroscopy can be marked bone seals and formations on the bone of the shoulder, inflammation of the periosteum.
Pain on movement
- Prolonged attacks of pain that do not leave a person even at rest. X-ray reveals changes in the joint.
tendonitis on x-ray
Important! It is necessary to seek help already at the first short-term pain sensations, since the development of the disease leads to the formation of complications.
Why is shoulder tendonitis dangerous?
In most cases, tendinitis resolves with timely medical attention. Pain and difficulty in movement subside.
Disease danger
If the treatment is delayed, then the pathology will eventually lead to complications, which are difficult or completely impossible to eliminate.
- Restriction of movement exacerbates inflammation, and also leads to a decrease in the size and performance of the delta and biceps.
- Inflammation of the tendon of the supraspinatus muscle can be the beginning of the development of ankylosis of the humeroscapular joint (immobility caused by the fusion of the articular surfaces of the scapula and humerus).
- Some types of tendonitis, such as supraspinatus tendonitis, can lead to thinning and partial or complete tendon rupture.
Do not ignore pain and bring inflammation to serious consequences
A traumatologist, orthopedist, surgeon can diagnose and select the necessary therapy regimen that will help cure tendonitis and remove the risk of developing unpleasant consequences.
Diagnostics
In most cases, inflammation of the tendons of the shoulder joint is determined already at the appointment. To do this, the doctor evaluates the nature of active movements, which usually cause pain, and therefore are limited. If the doctor himself moves the shoulder (passive movements), then pain does not occur or is not so intense.
Diagnosis of tendinitis
To make a final diagnosis and exclude other pathologies, additional examinations may be prescribed:
- with the help of MRI of the joint, areas of degeneration and rupture of the tendon are determined; Conducting MRI to detect the disease
- Ultrasound is used to detect ruptures and associated bursitis and arthritis; Ultrasound of the shoulder joint
- radiography and CR arthrography (X-ray with the introduction of contrast into the joint) reveal calcium inclusions and exclude arthrosis, fracture, dislocation and their consequences;
- arthroscopy - a study that consists in conducting a thin tube under anesthesia into the shoulder to examine the joint;
- the introduction of an anesthetic drug into the joint for tendinitis leads to pain relief, which is a diagnostic sign. Intra-articular injections in the shoulder to diagnose tendonitis
Laboratory methods for determining tendinitis do not play a special role.
Blood tests
Blood tests change only in severe degrees and in the presence of concomitant diseases:
- in the general blood test, an excess of leukocytes is observed during a bacterial process;
- with infectious inflammation caused by bacteria, the content of C-reactive protein in the blood increases;
- high concentrations of uric acid are noted with gout;
- rheumatoid factor is indicative of rheumatoid arthritis.
Diagnostics helps to identify the localization of inflammation, as well as the stage of the pathological process, which determines the treatment regimen.
- Diagnosis of tendinitis
- Calcific tendinitis
Source: https://med-explorer.ru/ortopediya/lechenie-ruk/tendinit-plechevogo-sustava.html
Chronic supraspinatus tendinitis occurs in people leading a rather active and mobile lifestyle.
In the movements of the shoulder joint, several muscles take part, each responsible for a certain movement. The supraspinatus muscle is responsible for abducting the arm to the side and to the side. Inflammation of the tendon of the supraspinatus muscle, the appearance of pain in the shoulder when the arm is moved to the side, and there is tendonitis of the supraspinatus muscle.
- 15 years experience treatment of diseases of the joints and spine
- All in 1 day– doctor’s examination, ultrasound, relieve pain and start treatment
- Doctor's appointment 0 rub until July 15th! in our treatment
Sign up for a free appointment
It is believed that supraspinatus tendonitis occurs most often in people who play sports professionally or lead a rather active and mobile lifestyle. Daily exhausting workouts take their toll.
However, even in people leading a completely measured lifestyle, inflammation of the tendon of the supraspinatus muscle may develop. A vivid example of this is the performance of unusual physical activity - washing windows, chopping firewood.
Such actions lead first to overload, and then to inflammation of the tendon.
Causes that can lead to the appearance of tendinitis:
- consequences of shoulder injuries;
- intense training and physical activity;
- bacterial infections in the shoulder area;
- rheumatic diseases.
In addition, it is also necessary to take into account the features of the anatomical structure of the shoulder joint of each person, which can lead to the appearance of the disease.
Inflammation often occurs where the bone and tendon of the supraspinatus connect. In the process of progression of the disease and maintaining the load on the shoulder, the adjacent tendons - the infraspinatus and subscapularis muscles of the shoulder - may also be involved in the inflammatory process. Very often, when examining patients with tendinitis of the supraspinatus muscle, tendonitis of these muscles is also detected.
The main symptom is pain in the tendon area with active movement of the shoulder - abduction of the arm to the side. The pain is localized in the region of the deltoid muscle, more along the anterior surface of the shoulder joint. Note that with passive movements, pain may not bother a person at all.
There are three stages of the disease:
I stage- there is only inflammation and swelling of the tendon of the supraspinatus muscle. Lasts up to 6 weeks.
II stage- movements in the shoulder joint, accompanied by a crackling sound and clicks. This is due to thickening of the tendon against the background of inflammation, and the appearance in its thickness of areas of scar connective tissue (fibrosis). Last up to 2-3 months
III stage- Calcium crystals are deposited in the tendon area. There is a pronounced limitation of movement in the joint. This condition is called calcific supraspinatus tendonitis. Sometimes in the area of the joint, you can notice a mild swelling of the tissues. It can last more than 1 year.
If you experience any of the symptoms, see your doctor for advice. He will prescribe you a course of treatment and help you get rid of the pain in the shortest possible time.
Book an appointment for supraspinatus tendinitis treatment
Diagnosis of supraspinatus tendinitis
- ultrasound diagnostics will show inflammation of the tendon of the supraspinatus muscle of the shoulder, swelling. More than 80% informative
- Radiography will show indirect signs - narrowing of the joint space, inflammation in the area of tendon attachment. The presence of calcium crystals and ossificates can be clearly seen.
- Analyzes will be uninformative
- Magnetic resonance imaging will show all the characteristic signs of supraspinatus tendinitis, will allow you to assess the condition of the joint capsule, the information content is 99%.
Methods for the treatment of tendonitis of the supraspinatus muscle
In order to get rid of the disease, first of all, it is necessary to create rest for the affected area of the body, eliminating all physical activity.
A fairly popular way is to introduce hormones - corticosteroids - into the affected area. Such drugs quickly relieve pain and eliminate the symptoms of the disease in a short time. Modern methods of physiotherapy - phonophoresis, myostimulation, traction therapy help to relieve the symptoms of inflammation of the tendon.
In the treatment of calcific tendonitis of the supraspinatus muscle, the method of shock wave therapy is effective - a sound wave causes the destruction of pathological tissues - scars and calcium crystals. This allows you to get rid of the cause of inflammation of the tendon completely.
In conclusion, I would like to note that you can use the services of our clinic. Stoparthrosis Medical Center specialized on treatment supraspinatus tendonitis. We offer more than 20 modern and non-surgical treatments. The efficiency of our methods is 95%. Every year we help more than 1,000 patients get rid of pain and return to a full life.
View all methods →
You can find out more about prices here
View all →
Feedback from our patients
“ We are sincerely grateful for every review left by you! ”
- Ermolaeva S.N. I want to express my sincere gratitude to the entire team of doctors for their professional and highly efficient work. I am already 83 years old, for the last 10 years I have been suffering from severe pain in my knee joints, which methods I have not tried, but they helped me here, thank you very much.
- Tsarev Alexander I went to them to crush a heel spur, my friends said that they would remove me in 3-4 sessions, in the end I did 7. But I really don’t know how much it helped, about 3 months have already passed, so far everything is fine. So thank you doctors.
- Doctor VK "Dynamo" Mamaev Yu.V. Over the years of cooperation, the team of doctors has repeatedly proved its high professionalism. I especially want to express my gratitude to the orthopedist Andrey Sergeevich Litvinenko, who is always ready to help.
- Doctor of HC “Tornado” Smirnov Yu.A. In professional hockey, injuries are inevitable, and injuries happen at least as often in women's hockey as in men's. And here, of course, you can not do without the help of a traumatologist and a physiotherapist. Many thanks to you colleagues.
- Raisa I came to the clinic with sore knees and back, they did a number of procedures, and these are shock wave therapy and plasma lifting, and you know, I felt relief from the first procedure, now I have finished one course, I feel good, but I think in half a year I need to will still be fixed. The clinic is very clean, everything is done with taste, everything is washed, you don’t sit in line for a long time, everything is on time. Many thanks to Andrei Sergeevich, this is a doctor from God, he is kind and sociable, he is always positive, and Irina Viktorovna thanks her very tender, caring, she will always come to ask if everything is fine with you, and Natalia A also thanks, the whole staff is excellent. I advise everyone with such problems to go to this clinic.
- Vorobieva O.V. Thanks to the doctors of this medical center!!! I am 56 years old. I have been an accountant all my life. I suffered from cervical osteochondrosis for a very long time, I woke up at night from numbness of my fingers, my head often hurt. On the Internet, I accidentally stumbled upon your site, called and underwent a course of treatment. Now I feel comfortable, my headaches are gone and there is no numbness in my hands at night.
- Natalya Anatolyevna I suffered with heel pain for 2 years. I went through a physio-laser, a magnet and injections in the heels. The relief is slight. Only after the course of the shock wave did I forget about the excruciating pains in this area. Special thanks to Irina Viktorovna, who performed the shock wave procedure on me. Competent, charming, subtly feeling the pain and suffering of patients. Pleasant sunny voice and qualified approach to his work. I sincerely thank you for your help.
Three simple steps to your health
Make an appointment
Source: http://stopartroz.ru/what-a-treat/pain-in-the-shoulder/supraspinatus-tendinitis.html

The term tendonitis defines an inflammatory process that develops in the ligaments and tendons of various structures of the human musculoskeletal system. Inflammation of the tendon of the supraspinatus muscle, which is part of the shoulder cuff, is a fairly common phenomenon that develops under the influence of various provoking factors.
If a medical specialist has diagnosed tendinitis of the supraspinatus muscle of the shoulder joint, the treatment is selected individually, depending on the etiology (origin) and severity of the course of the disease.
Structural features
The shoulder joint has a round shape, which allows a high range of motion in 3 different planes.
The structure that increases strength and stabilizes the joint is the cuff. It includes rotational, supraspinatus, infraspinatus, subscapularis muscles.
The supraspinatus tendon is attached to the lesser tubercle of the humerus, it passes in close proximity to the capsule.
Features of the anatomical structure determine the frequent combined inflammation of the tendon of the supraspinatus muscle and other components of the shoulder, consisting of their soft tissues.
The pathological process extends to the biceps tendon (biceps).
After determining the prevalence of inflammation that accompanies tendonitis of the tendon of the supraspinatus muscle of the shoulder joint, treatment and rehabilitation are selected by the doctor in accordance with the results of the study.
Etiology
Inflammation is a complex pathophysiological reaction that develops as a result of tissue damage.
In the area of the pathological process, cells of the immune system accumulate, which produce certain biologically active compounds (prostaglandins) that respond to the characteristic manifestations of the inflammatory reaction (pain, tissue swelling, hyperemia). The main provoking factors leading to inflammation are:
- Intensive exercise on the shoulder.
- Postponed injuries that affect the cuff to varying degrees (fall on an outstretched arm, bruise, dislocation, fractures of the upper third of the humerus).
- Infectious inflammation, which is the result of the vital activity of pathogenic (pathogenic) or opportunistic microorganisms.
- Aseptic inflammation that develops against the background of local hypothermia of the shoulder area.
- The autoimmune process is a pathology of the immune system, in which antibodies are "erroneously" produced against one's own tissues, in particular the structures of the musculoskeletal system.
- Degenerative-dystrophic processes in which the nutrition of the tissues of the structures of the musculoskeletal system is disturbed, leading to their destruction with the subsequent development of an inflammatory reaction.
After the doctor has diagnosed the tendinitis of the tendon of the supraspinatus muscle of the shoulder, the treatment is prescribed with the obligatory consideration of the causes that led to the inflammation.
Manifestations
The main clinical sign of the development of inflammation of the tendon of the supraspinatus muscle is pain. Its intensity can be different, depending on the cause, severity and stage of the disease.
Pain usually intensifies during attempts to perform hand movements in the shoulder.
In a severe course of the disease, swelling of the tissues with an increase in the joint in volume, as well as reddening of the skin (hyperemia), attracts attention.
Diagnostics
Regardless of the origin, most diseases of the components of the shoulder joint have a similar clinical picture. A reliable determination of the degree of changes is carried out using various modern imaging techniques (X-ray, tomography, arthroscopy, ultrasound). To determine the cause of inflammation, a laboratory test is prescribed.
Based on the results, allowing to establish the diagnosis of tendinitis of the supraspinatus muscle of the shoulder, the treatment is prescribed by the orthopedic doctor. In autoimmune pathology, the diagnosis and prescription of therapeutic measures is carried out by a rheumatologist.
Treatment
After the conclusion of supraspinatus tendonitis has been made, the treatment is determined by the complex. It includes several therapeutic areas, which include conservative techniques, as well as the performance of a surgical operation. After the main course of therapy, rehabilitation measures are prescribed.
Conservative tactics
Conservative tactics means non-surgical treatment with the help of medications. For this, non-steroidal anti-inflammatory drugs are prescribed, which can reduce the severity of the inflammatory reaction.
In autoimmune inflammation, hormonal anti-inflammatory drugs are also prescribed, which reduce the activity of the immune system. Prolonged inflammation requires physiotherapeutic procedures (electrophoresis, magnetotherapy, ozocerite).
Surgery
The appointment of the operation is carried out with pronounced tissue changes, which are usually the result of prolonged and severe inflammation. Mostly plastic surgery of altered tissues is performed. Access to the supraspinatus tendon can be open (wide incision) or performed using arthroscopy (introduction through small incisions of an arthroscope with microinstrumentation).
Rehabilitation
After the main course of treatment, rehabilitation measures are prescribed. They include therapeutic exercises that improve the functional state of the shoulder, as well as adapt the ligaments and tendons to physical activity. The duration of rehabilitation varies within about six months, which depends on the severity of the inflammatory reaction.
Prevention
Preventive measures are aimed at preventing the re-development of the inflammatory response. They consist in the implementation of recommendations regarding the limitation of excessive loads, hypothermia, as well as injuries.
Shoulder tendinitis is a common inflammatory and degenerative pathology of the shoulder joint, not directly related to acute shoulder injury. Prolonged high loads on the shoulder cause microtrauma of the muscle tendons that form the capsule of the shoulder joint, their inflammation and subsequent degeneration.
Tendinitis is an inflammatory process that develops in the tendons or tissues that connect muscles to bones. Most often, the process is localized in the place where the bone is in contact with the tendon, the development of pathology can go along the tissues. Anyone can be affected by the disease, and there are no differences by gender, profession or age.
Tendinitis refers to periarticular diseases and can be combined with other similar pathologies:
- enthesitis - inflammation of the tendon at the place of its attachment to the bone;
- tenosynovitis - simultaneous inflammation of both tendons and bags;
- bursitis - inflammation of the joint cavities and bags surrounding the tendons.
Bursitis or synovitis usually precedes tendinitis.
Mechanism
The capsule of the shoulder joint is formed by 5 muscles: the supraspinatus, teres minor, infraspinatus, subscapularis (form the rotator cuff of the shoulder) and the large biceps (biceps). Since the cavity of the shoulder joint only partially covers the head of the shoulder, the load when holding it in the correct position and during movements falls on the muscle tendons.
To stabilize the shoulder and prevent displacement of the humeral head, the joint is reinforced with cartilaginous lips (structures that increase the depth of the glenoid cavity), ligaments, as well as muscles and their tendons that form the rotator cuff.
In case of excessive mechanical impact, trauma to the structures of the rotator cuff can occur. With a sharp abduction of the entire arm, as well as flexion of the upper limb in the elbow joint, a rupture of the distal tendon of the biceps brachii muscle is possible, which requires longer treatment and rehabilitation.
The pathogenesis of the development of changes in the structures of the musculoskeletal system, including the cuff, consists in the implementation of 2 mechanisms:
- Significant force acting on the shoulder, as a result of which pressure is exerted on the structures of the cuff by the head of the humerus.
- Decrease in the strength of the fibers of the structures, which primarily affects the tendon. In this case, damage can develop against the background of normal loads.
Elucidation of the mechanism of development, due to the implementation of which damage to the supraspinatus muscle of the shoulder joint occurs, makes it possible to select the most effective therapeutic tactics in the future.
A rupture of the supraspinatus muscle of the shoulder develops as a result of the implementation of a pathogenetic mechanism, the essence of which is an excessive impact, the force of which is aimed at lengthening the tendon (stretching).
More pronounced changes in the fibers are formed against the background of degenerative or inflammatory changes. In this case, the trauma suffered is more severe, it affects several components of the shoulder at once.
Main reasons
The shoulder joint has a complex structure, which allows you to make movements in a large volume. The articulation forms the head of the humerus, which is immersed in the glenoid cavity of the scapula.
Around the bones are tendons and ligaments that form the rotator cuff of the shoulder and hold the joint in a physiological position.
The cuff consists of the tendons of the subscapularis, infraspinatus, small round, supraspinatus muscles of the shoulder and the long head of the biceps. Under the influence of adverse factors, the rotator cuff can be damaged by the acromioclavicular joint, the coracoacromial ligament, or the anterior part of the acromion during movements of the upper limb.
A pathological condition that is accompanied by inflammation of the tendons and other soft tissues of the shoulder joint is called tendinitis.
The supraspinatus tendon, biceps tendon, and articular capsule may be involved in this process.
But the main lesions are the junction of bones with ligaments.
The disease is very common among the adult population and among athletes who once suffered a shoulder joint injury.
Elderly women are affected much more often than men. This is directly related to hormonal disorders of the menopause.
Constant overstrain of the shoulder girdle due to intense physical activity causes the appearance of microtraumas of the tendons of the supraspinatus muscle, which leads to the launch of the inflammatory process in them - tendinitis. Most often it is provoked in athletes due to the friction of the tendons on the bone during exercise.
The most common causes of the disease include:
- Large physical load on the shoulder joint for a long time;
- Misformed tendons;
- Features of the anatomical structure of people, for example, limbs of different lengths;
- The presence of various injuries associated with the shoulder joint;
- Infectious processes caused by the presence of various kinds of bacteria in the body;
- The presence of rheumatic diseases such as arthritis or gout;
- Incorrect posture;
- Allergic reactions of the body to certain drugs.
Rupture of the tendon of the shoulder muscle is a polyetiological pathological condition, the development of which can be caused by several provoking factors, which include:

Finding out the main factor that led to the injury of the ligaments and tendons of the shoulder joint, allows the doctor not only to choose the most optimal treatment, but also to take measures to prevent its re-development.
Classification
The following types of shoulder tendon pathologies are diagnosed:
- rotator cuff tendonitis: supraspinatus, infraspinatus, round and subscapularis;
- biceps tendonitis (biceps tendonitis);
- calcific tendinitis;
- partial or complete rupture of tendons.
The risk group is made up of people who are over forty, athletes and those who constantly work physically. Microcracks appear due to frequent or constant load on the same hand.
Most often in the shoulder joint are affected:
- biceps tendon;
- shoulder joint capsule;
- supraspinatus muscle.
This traumatic or pathological injury to the ligaments of the shoulder is classified into types according to several criteria. Based on the severity of the violation of the anatomical integrity, a complete (injury affects all layers of the tendon) and partial rupture of the tendons of the shoulders are distinguished. Incomplete damage to the fibers without disturbing the overall anatomical structure is also called stretching.
According to the localization of the injury, several main varieties are distinguished: rupture of the tendon of the biceps muscle of the shoulders, supraspinatus and infraspinatus muscles, small round and scapular muscles.
The location of traumatic or pathological damage to these structures of the musculoskeletal system mainly depends on the direction of the impact of excessive mechanical force on the shoulder. According to the etiological principle (a group of provoking factors that led to a violation of the anatomical integrity of the connective tissue structures), traumatic and pathological damage is distinguished.
The classification of this type of injury or pathological integrity violation allows the doctor to determine its type and prescribe adequate treatment.
.
Injury to the tendon of the supraspinatus muscle of the shoulder joint is classified according to several criteria that are clarified during the diagnostic process. Depending on the degree of change, there are:
- Partial supraspinatus tendon injury is a milder form of trauma in which the overall structure and shape is preserved. There is a rupture of individual fibers, the total length of the tendon increases, so this damage is also called sprain or intratendinous damage to the tendon of the supraspinatus muscle.
- A complete rupture of the tendon is usually in the region of the lesser tubercle of the humerus, which is accompanied by a violation of the form and function.
- Combined changes in which the joint capsule is affected.
According to the main mechanism of changes and the group of provoking causal factors (pathogenetic and etiological criteria), 2 forms of changes are distinguished:
- Degenerative damage to the tendon of the supraspinatus muscle of the shoulder is a violation of integrity, which in most cases is the result of malnutrition of connective tissue structures.
- inflammatory changes.
- Post-traumatic violation of the integrity, occurring against the background of unchanged structures.
There are also 3 degrees of severity of the pathological condition. The division of changes in the structures of the cuff allows the orthopedist-traumatologist to choose the optimal therapeutic tactics and subsequent rehabilitation.
An isolated change is also distinguished, affecting only the tendon of the supraspinatus muscle, and a combined injury, in which other structures of the shoulder are involved in the process to varying degrees.
Provoking factors
A significant effect of force on the shoulder can be in various situations, which include falls on an outstretched arm, excessive extension, and blows. The decrease in the strength of the fibers is the result of the development of pathological processes:
- Degenerative-dystrophic pathology, which is the result of malnutrition of cartilage structures with their subsequent destruction.
- Inflammatory conditions - tissue damage is due to the development of an infectious, autoimmune (the appearance of antibodies to one's own tissues that damage the structures of the musculoskeletal system) process.
- Congenital change in the properties of the connective tissue structures of the body, which has a genetic hereditary origin.
Elucidation of the main cause that led to changes in the structures, in particular the supraspinatus muscle, is necessary for the choice of preventive measures in the future.
Symptoms and signs
The rupture of the supraspinatus muscle is manifested by quite characteristic symptoms, which include:
- Sharp pain that appears immediately after an injury. In the case of gradual damage to the fibers against the background of the pathological process, pain may increase gradually.
- Increased discomfort during movements in the shoulder, especially when trying to raise the arm up.
- Violation of the stabilization of the joint, in which habitual dislocation can develop with frequent exit of the head of the humerus from the articular cavity against the background of normal loads.
- The appearance of inflammatory signs - damage is accompanied by inflammation of tissues and ligaments (tendinitis) with reddening of the skin, its swelling and an increase in the shoulder in volume.
The severity of clinical signs of tendon fiber rupture depends on the severity of the pathology.
Symptoms
A clear sign of shoulder tendinitis is the appearance of a sharp pain in the damaged joint during active movement and the presence of swelling on its surface. The pain in this case can be of a different nature - from acute to dull and aching.
Probing the intertubercular furrow also causes pain. Contracture (limited mobility due to constriction of soft tissues) of the joint significantly reduces the range of any movement of a person.
The symptoms of calcific tendonitis are more varied. then not only sensations of pain, but also a certain stiffness, limited possibilities in the movements of the shoulder. A sign of this tendinitis is the appearance of a crunch in the shoulder when the arm is moved.
In some cases, no symptoms are observed at all.
Rotary tendonitis can be distinguished by pain when the arm is raised up or thrown forward sharply. A progressive disease does not allow even minor movements to be made: to squeeze a hand or push something, to get a book from a shelf without experiencing pain.
The later stages are characterized by sensations of pain both during the movement of the arm and in its calm state. Often the pain is given in the elbow joint, there is a mild swelling.
Such clinical manifestations affect the function of the shoulder joint. They bring significant discomfort, lead to a decrease in a person’s ability to work and force them to seek qualified medical help.
The clinical picture of changes includes several rather characteristic manifestations:
- Pain in the shoulder area, the intensity of which depends on the severity of the changes. After an injury, the pain is acute, in the case of the development of a pathological process (inflammation and degenerative-dystrophic process), it develops and intensifies gradually.
- Limitation of active movements - it is difficult for the patient to withdraw the arm, this is especially noticeable when the arm is abducted by 60 °.
- The appearance of signs of an inflammatory reaction, which include reddening of tissues due to increased blood flow, swelling with the release of the liquid part of the blood into the intercellular substance, as well as pain associated with direct irritation of sensitive nerve endings.
The appearance of several signs of changes in the integrity of the structures of the cuff significantly reduces the quality of life of a person and is the basis for contacting the appropriate medical specialist.
Diagnostics
The diagnosis is made on the basis of the clinical picture. Tendinitis most often has to be differentiated from traumatic injury to the rotator cuff of the shoulder.
The difference is revealed by assessing the range of motion: with tendinitis, the volume of passive and active movements is the same, with damage to the rotator cuff, there is a limitation in the range of active movements compared to passive ones.
In doubtful cases, the patient is referred for an MRI of the shoulder joint. With tendinitis, MRI shows a thickening of the tendon sheaths and the joint capsule, with a traumatic injury, a rupture site is visible.
To exclude other diseases and pathological conditions (arthrosis, consequences of a fracture or dislocation), an x-ray of the shoulder joint is prescribed. In the absence of calcification, the radiological picture is within the normal range. With calcific tendovaginitis, areas of calcification are visible on the pictures.
When the first clinical signs of the disease appear, it is necessary to consult a doctor to diagnose the pathological process. The earlier the disease is detected, the faster you can achieve recovery and reduce the likelihood of tendinitis becoming chronic.
Diagnosis of the disease includes the following steps:
- collection of patient complaints (nature of pain, possible causes of the disease, concomitant pathology);
- examination of the patient (listening to breathing, heart sounds, feeling the shoulder joint and surrounding muscles;
- checking the volume of passive and active movements of the affected upper limb);
- laboratory diagnostics (general analysis of blood and urine);
- instrumental diagnostics (radiography, ultrasound, CT, MRI);
- arthroscopy.
Based on the results of the diagnosis, the doctor makes the final diagnosis and determines the treatment tactics. In the general blood test, signs of inflammation (high ESR, leukocytosis) are revealed, and the formation of calcifications is detected on the x-ray.
The most informative is computed (CT) and magnetic resonance (MRI) tomography, which allows you to determine pathological changes in the tendons and soft tissues.
Ultrasound examination (ultrasound) helps to study the state of the internal structures of the joint, ligaments, muscles, blood vessels and to conduct a differential diagnosis with other diseases. Arthroscopy is performed using endoscopic equipment, which makes it possible to directly examine the affected anatomical structures.
In order to get rid of the disease, first of all, it is necessary to create rest for the affected area of the body, eliminating all physical activity. A fairly popular way is to introduce hormones - corticosteroids - into the affected area.
Such drugs quickly relieve pain and eliminate the symptoms of the disease in a short time. Modern methods of physiotherapy - phonophoresis, myostimulation, traction therapy help to relieve the symptoms of inflammation of the tendon.
In the treatment of calcific tendinitis of the supraspinatus muscle, the method of shock wave therapy is effective - a sound wave causes the destruction of pathological tissues - scars and calcium crystals. This allows you to get rid of the cause of inflammation of the tendon completely.
Tendonitis is diagnosed mainly by visual inspection. It is sometimes differentiated from a rotary shoulder cuff injury. They are distinguished only by the volume of passive and active movements, which is the same with tendonitis, and different (less active) with an injury to the rotator cuff.
The clinical picture makes it possible to suspect the presence of a pathological or traumatic lesion of the shoulder. To clarify the degree of severity, the location of areas of violation of the anatomical integrity, objective diagnostics is used using various methods for obtaining images of internal structures.
To date, good medical centers use radiography (the study is performed in different projections), MRI, CT, ultrasound diagnostics and arthroscopy. The choice of technique is determined by the results of the clinical examination (survey, examination, palpation of tissues and the performance of diagnostic tests), as well as the technical capabilities of the diagnostic department of the medical institution.
Radiography
In the trauma center immediately after the treatment of the injured person, X-rays are most often performed. The method allows to visualize gross violations of the anatomical integrity and ratio of the bone structures of the shoulder joint (bone fracture, dislocation) and its ligamentous apparatus.
Since the human body is exposed to radiation exposure during radiography, this study may not be performed for all categories of patients (pregnancy and breastfeeding are medical contraindications for x-rays).
Tomography
Computed tomography or magnetic resonance imaging are tissue imaging techniques with layer-by-layer scanning. This makes it possible to detect even small changes in them. The performance of these studies is accompanied by a lower radiation exposure. Tomography is often performed to diagnose pathological changes in the tendons that led to their rupture.
Ultrasound examination (ultrasound) is a safe technique for imaging various structures, in which the patient's body is not exposed to radiation exposure. The main indication for ultrasound of the shoulder joint is the detection of inflammatory changes in the tissues, as well as the determination of the volume of synovial fluid (an increase in the volume of synovial fluid in the joint cavity indicates a pronounced inflammatory reaction).
Arthroscopy
Most changes in the structures of the musculoskeletal system are accompanied by similar clinical symptoms. Therefore, a reliable clarification of the etiology, the degree of changes is performed using diagnostic techniques.
Modern research methods include visualization of the structures of the musculoskeletal system using radiography or fluoroscopy, endoscopic techniques (arthroscopy), tomography (methods with a high separation power of imaging), ultrasound examination.
To determine the cause of the disease, as well as to determine the severity of functional changes, laboratory tests are prescribed.
.
In order to reliably determine the location, nature and severity of the injury, the orthopedic traumatologist prescribes an additional examination. It includes techniques to visualize internal structures.
These include radiography, tomography with layered tissue scanning (visualization of tissues can be carried out using X-rays or the effect of resonance of the nuclei of atoms in a magnetic field), ultrasound of the components of the musculoskeletal system, as well as arthroscopy (a minimally invasive diagnostic and treatment technique).
The choice of examination method is determined by the results of the examination by the doctor, as well as the technical capabilities of the medical institution.
.
Treatment
Effective treatment of tendinitis of the shoulder joint helps a complex effect on the pathology. In this process, not only medical manipulations are important, but also a deep understanding by the patient of the essence of the disease.
As a rule, various methods of treatment are used:
- Medical therapy.
- Physiotherapy.
- Therapeutic gymnastics.
- Massage.
- Operation.
The choice of one method or another is based on the characteristics of the course of the disease and the properties of the organism. Therefore, the therapeutic program is developed individually for each patient.
At the same time, special attention is paid to unloading the affected shoulder and creating rest. The factors that provoke the appearance of pain should be eliminated as much as possible, up to wearing a scarf bandage. However, prolonged immobilization of the joint is not recommended.
Therapeutic measures for tendinitis of the shoulder depend on the stage of the pathology.
At stage I of the development of tendinitis, it is enough to temporarily eliminate the load on the shoulder and limit its mobility (immobilization). Pain-causing movements should be avoided for 2-3 weeks. Therapeutic exercises to strengthen the muscles of the shoulder and increase mobility are carried out with a gradual increase in load.
Also shown are drugs of the NSAID group inside for up to 5 days and topically. Local therapy with NSAIDs and carried out for 2 weeks. during the acute period. With a protracted course, ointments that improve blood flow (with capsaicin, etc.) are effective.
Stage II requires supplementing treatment with injections into the joint cavity (lidocaine, bupivacaine in combination with triamcinolone). Anesthetics with a short action are used in the diagnosis of pathology, for a therapeutic effect, drugs with a long action are used. Muscle relaxants are used only for pronounced pain and in rare cases (a lot of side effects).
Physiotherapeutic procedures accelerate recovery: electro- and phonophoresis, magnetic currents, cryotherapy, laser treatment, ultrasound and paraffin applications.
At stage III, with the above treatment, resection of the anterior part of the acromial process is performed. Surgical removal of scar tissue and partial excision of tendon aponeuroses is indicated when conservative measures fail and vasoconstriction develops.
In the case of more severe forms of the lesion, treatment of tendinitis of the shoulder joint begins with conservative therapy using anti-inflammatory drugs. If calcific tendonitis is diagnosed, then a procedure is performed to remove salt deposits.
To do this, two needles with a large hole are inserted into the joint and salt is washed out with the help of saline. Then cold therapy, massages, physical procedures, and therapeutic exercises are added. If such measures do not lead to a positive result, then one has to resort to surgical methods of treatment.
In this case, it would be appropriate to use an arthroscope - a medical device equipped with a video camera. It is introduced into the lumen of the joint and the necessary manipulations are carried out. But a classic strip operation can also be carried out.
The period of postoperative rehabilitation usually reaches two to three months, but it will be possible to return to the usual active life no earlier than in three to four months.
Without the use of medicines, it is difficult to imagine the treatment of any pathology, including tendinitis. The drugs are used to reduce inflammation, relieve pain and swelling, eliminate muscle tension and improve the function of the shoulder joint.
Given the great importance of degenerative processes in the development of the disease, one should also include those drugs that will improve metabolic processes in the tendon itself, contributing to its healing.
The introduction of corticosteroid drugs into the lesion has a positive effect. Soreness at the same time quickly goes away along with the inflammatory process.
Injections cannot completely cure a person, but they can completely reduce the rate of collagen production and its degradation. Due to this, the level of strength is reduced, which can result in a break. In this regard, this treatment option for tendinitis is justified in the acute period, no more than once every 2 or 3 weeks.
On the positive side, non-steroidal anti-inflammatory drugs that are taken orally have proven themselves. But taking them for a long time is recommended for a chronic state of overexertion. The appointment of analgesics and muscle relaxants is justified.
The effect brings the use of gels and ointments that contain non-steroidal anti-inflammatory drugs. In some cases, they can replace systemic tablets.
- Anti-inflammatory (Artrozan, Dicloberl).
- Muscle relaxants (Mydocalm).
- Chondroprotectors (Artra, Don).
- Vascular (Solcoseryl).
- Vitamins and microelements.
- Hormones (Diprospan, Kenalog).
- Local anesthetics (Novocain).
The last two groups of drugs are used exclusively for topical use. They are injected into the area of the affected tendon to eliminate pain. Various anti-inflammatory ointments (Dolobene, Diklak) are used as local therapy.
Medicines should be used in accordance with the doctor's prescriptions. Self-administration of drugs is strictly prohibited due to the possibility of developing unforeseen reactions.
Good additional help can also be provided by traditional medicine, which has analgesic and anti-inflammatory properties:
- Curcumin is effective in the treatment of tendonitis, which, at a daily dosage of half a gram, is taken with food as a seasoning. He declared himself as an excellent remedy that relieves pain, copes well with inflammation.
- Bird cherry fruits insist in a glass of boiled water and drink two to three times a day as tea. The tannins of the berries perfectly relieve inflammation and have a strengthening effect on the body.
- A glass of assembled partitions of Volotsk (walnut) nuts is poured with half a liter of vodka. Insist in a dark place for three weeks. 30 minutes before a meal, take 30 drops of tincture with a large volume of chilled boiled water.
- An infusion made from a mixture of two components showed itself perfectly: sarsaparilla root and ginger root taken in equal proportions. A teaspoon of the crushed composition is poured into a glass of boiling water and drunk instead of tea.
- It is advisable to drink tea twice during the day.
- On the first day after the injury, a cold compress should be applied to the sore spot, and on the following days, warming therapy is preferable.
Sprains are a very common injury to the shoulder joint. Sprain leads to rupture of the tendons, which leads to severe pain. This may be due to a large joint overload. Thus, the problem is most common in athletes, weightlifters and people who perform hard work.
The more the victim delays with treatment, the worse it can affect his condition, since the disease can progress rapidly. A simple shoulder sprain can develop into shoulder bursitis.
Tendon rupture must be differentiated from shoulder dislocation. Since the shoulder is a moving part of the body and is not always stable in some positions, tissues can be damaged.
Such injuries can lead to chronic consequences for the shoulder joint. The thing is that the muscles that surround the shoulder joint are considered to be the holding back of the shoulder.
Often, shoulder inflammation begins to develop with tendobursitis (catarrh of the tendon bag) and tendosynovitis (tendovaginitis, catarrh of the shoulder joint sheath).
Only after the manifestation of the first signs of the inflammatory process, the disease passes into the region of the muscle and tendon. This complication is diagnosed as tendonitis of the shoulder joint.
Causative agents of tendinitis of the shoulder joint
There are many reasons that can provoke the awakening and further development of inflammatory processes in the human body. To defeat the disease, you need to have a clear and accurate understanding of its etymology and how to treat it.
There are several reasons for the development of tendinitis:
- The first risk group of people who are susceptible to this disease include basketball players, tennis players, handball players, hammer or javelin throwers, gymnasts.
- The second are people with professions that require significant physical output and heavy workload. Almost everyone involved in construction work (masons, plasterers), drivers of vehicles (truckers, taxi drivers) and others.
- Injuries and microtraumas due to an active lifestyle.
- People with both acquired and congenital disorders of tendon development (loss of elasticity and elasticity of the muscle).
- Problems with the spine.
- Various infectious diseases that spread through the bloodstream and affect the weakest places in the body. The reason for this is poor ecology and pathogenic flora.
- Various stressful situations, depressive states lead to muscle spasms and additional stress on connective tissues.
- Taking medications and an allergic reaction to them can provoke inflammation of the shoulder joint.
- Hereditary or acquired joint dysplasia. Thyroid disease or diabetes.
- Reduced immunity.
- Prolonged stay with a tight bandage or plaster.
- Incorrect restorative therapy in the process of rehabilitation from surgical intervention in the area of the shoulder joint.
- Shoulder tendinitis may be associated with anatomically incorrect development of the shoulder joint, its degradation, which forms a focus of inflammation.
- Exposure to cold rain, prolonged exposure to drafts and other adverse climatic conditions.
Osteochondrosis of the cervical region; rheumatoid arthritis; osteoporosis (bone fragility); failure in metabolic processes (gout) and many others chronic diseases have a negative effect on the departments of bone, muscle and connective tissues.
Symptoms of shoulder tendonitis
First of all, as with any inflammatory process, tendinitis of the shoulder joint is accompanied by pain. There are several manifestations:
- The primary symptom is aching pain during movement, but with further development it will remind of itself even at rest.
- Hyperemic areas of the epidermis will appear (reddening of the skin, with pressure on them, muscle compaction and fever are felt).
- Clicks will be heard when moving, even without a special device (phonendoscope).
- In rare cases, there is a slight swelling, which causes slight inconvenience and reduces the mobility of the joint. It will be difficult for the patient to take objects located at a height, clothes may become narrow at the shoulders.
- Over time, the pain may move to the elbow joint and begin to reveal itself during sleep.
- The pain syndrome can manifest itself both in the form of a sharp backache, and a long, monotonous aches.
If the problem is ignored for a long time, the patient is threatened with partial or complete atrophy of muscle tissue in the shoulder region. It is quite difficult to treat such a pathology, and sometimes it is simply useless.
Salt deposits in the shoulder joint
Due to an improper lifestyle or certain diseases, the tendons of the shoulder area are exposed to salt deposits in them. In such cases, doctors diagnose calcific tendonitis of the shoulder joint.
Several muscle groups take part in the movements of the shoulder joint, each of which is responsible for a certain direction of movement. The supraspinatus muscle is responsible for abducting the shoulder to the side, inflammation of the tendon of the supraspinatus muscle, accompanied by the appearance of pain in the shoulder, is called supraspinatus tendinitis.
Who is most at risk for tendinitis?
It is believed that supraspinatus tendonitis affects people who play sports professionally, as well as those who have a fairly active and mobile lifestyle. Daily exhausting workouts take their toll.
However, even people who see a completely measured lifestyle can develop inflammation of the tendon of the supraspinatus muscle, for example, when performing unusual physical activity - washing windows, chopping firewood, etc., that is, a load that is not performed daily by a person and is considered quite critical for him.
Moscow, st. Berzarina 17 bldg. 2, Oktyabrskoye Pole metro station
Moscow, st. Koktebelskaya 2, bldg. 1, metro Boulevard Dmitry Donskoy
Moscow, Bolshoi Vlasevsky lane 9, Smolenskaya metro station
Make an appointment
In 2009 he graduated from the Yaroslavl State Medical Academy with a degree in general medicine.
From 2009 to 2011, he underwent clinical residency in traumatology and orthopedics at the Clinical Emergency Hospital named after. N.V. Solovyov in Yaroslavl.
From 2011 to 2012, he worked as a traumatologist-orthopedist at the emergency hospital No. 2 in Rostov-on-Don.
Tendinitis has 3 stages of the disease, determined by the radiograph, in accordance with which treatment is prescribed.
- First stage. At the initial stage, outpatient treatment is prescribed with recommendations for limited movements in the affected limb. But immobilization of the joint (maximum immobilization) is contraindicated, because in this case, inflammatory processes in it, the development of adhesive arthritis are possible. To relieve the sensation of pain and eliminate the inflammatory process in the shoulder joint, an orthopedist prescribes anti-inflammatory drugs. Physiotherapy exercises complete this stage of treatment. They are aimed at returning the normal functioning of the shoulder joint and strengthening muscle groups.
- Second stage. If this stage of the disease is detected in a patient, then the treatment is supplemented with glucocorticoids and local anesthetics, which are administered intraarticularly. The first drugs relieve the inflammatory process in the tendon, and the latter allow you to achieve rapid pain relief.
- Third stage. The advanced stage of tendonitis is the most difficult to treat. The procedures performed at the previous stages are ineffective here. There is a need to remove (resection) part of the acromion. Sometimes shoulder redressing is indicated under general anesthesia, in which the doctor "breaks" the joint capsule, which makes it possible to increase the range of motion. An operation is also performed to cut the capsule and rotator cuff, which can be in the classical version (open access) and arthroscopic (small incision). After the operation, physiotherapeutic procedures and exercise therapy are again prescribed, and the rehabilitation period, as a rule, lasts up to three months. Treatment of calcific tendinitis consists in the elimination of calcareous formations and inflammatory processes in the shoulder. It can be done conservatively or surgically.
If the form of the disease is defined as mild, then the following procedures are limited:
- Electrotherapy (removal of pain syndrome).
- extracorporeal shock wave therapy (exposure to the diseased area of low-frequency pulses with increased vibration).
- Subacromial infiltration (intense pain relief).
- Ultrasonic massage (providing enzyme activation and improving the supply of cells with oxygen).
- Washing of the joint (using the method of puncture, the joint is washed, which allows the removal of calcareous formations).
If the desired effect is not achieved with such treatment, then the orthopedist prescribes surgery, during which an incision is made and the lime mass is removed through it.
Ecology of life. Health: The supraspinatus is a small, thick muscle that sits in a horizontal depression at the top of the shoulder blade. The supraspinatus stabilizes the shoulder joint and works in conjunction with the deltoid to raise the arm to the side.
The supraspinatus is a small, thick muscle that sits in a horizontal depression at the top of the shoulder blade. The supraspinatus stabilizes the shoulder joint and works in conjunction with the deltoid to raise the arm to the side.
Like the other muscles of the rotator cuff group, it is attached to the top of the humerus. Its deep location under the fibers of the upper part of the trapezius muscle makes probing somewhat difficult.
The causes of pain in the supraspinatus muscle are the same problems as in the infraspinatus muscle (carrying weights in the hands, keeping from jerking forward). Tension points in this muscle are usually broken in combination with restriction of movements in the trapezius and infraspinatus muscles.
Rowers and weightlifters are particularly susceptible to this hazard. The pain usually appears in the upper part of the shoulder, right in the middle part of the deltoid muscle. She gives down to the shoulder, sometimes to the forearm and the outside of the elbow. If there are tension points in the supraspinatus muscle, you will not be able to raise your hand to shave or comb your hair, put your hand in your back pocket, fasten a button at the back.
In the supraspinatus muscle, it is somewhat difficult to locate the tension points due to the location of the muscle under the trapezius muscle. You will most likely need the help of another person who, by acting on the tension points, will improve the condition of the muscle, which requires strength.
Sit on a chair, lean against its back and slouch a little. This will allow the trapezius muscles to relax and make it somewhat easier to feel for points of tension in the supraspinatus muscle.
Feel for the acromion, a. then follow back along the spine of the scapula. When you reach the free edge of the bone near the spine, move your hand about 2.5 cm to the top of the shoulder. Press firmly on the trapezius muscle here to feel the tense and very painful area.
This will be one of the points of tension of the supraspinatus muscle. Press on it for 20-30 seconds, and gradually you will feel relief. Then, if you move your hand 2.5 cm to the top of the shoulder, you can feel another tense painful point. Treat her the same way.
Stretch 1: put your hand behind your back at waist level. Grab the wrist of the injured hand with the other hand and gently pull the arm across the waist and then up. Hold this position for 15-20 seconds.
The scapula and humerus take part in the formation of the shoulder joint. Therefore, first of all, it is advisable to consider the anatomical formations of these bones associated with the topography of the shoulder joint. The outer angle of the scapula is represented by the articular cavity(cavitas glenoidalis), above and below, which are located supraarticular(tuberculum supraglenoidal) and subarticular (tuberculum infraglenoidale) tubercles. On the upper edge near the outer corner is the coracoid process(processus coracoideus), medial to which there is a notch of the scapula(Incisura scapulae). The coracoid process and subarticular tubercle are separated from the glenoid cavity of the neck of the scapula(collum scapulae). Blade spine (spina scapulae), goes into acromion(acromion) having an angle (angulus acromialis).


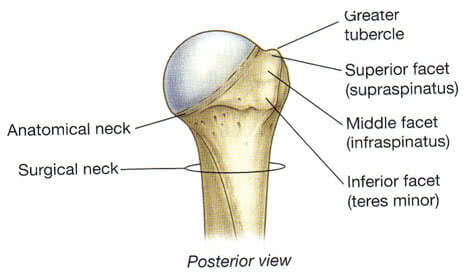
AT proximal end of the humerus (oshumerus) distinguish head, anatomical neck, large and small tubercles, intertubercular groove, surgical neck. Humeral head (caputhumeri) covered with hyaline cartilage. Anatomic neck (withllitanatomicum) separates the head of the humerus from the rest of it. Large tubercle { tuberculummajus) located on the lateral surface of the humerus and serves as the site of attachment of the supraspinatus (t.supraspinatus), infraspinatus (t.infraspinatus) and teres minor (t.teresmajor), providing external rotation of the shoulder. Lesser tubercle (tuberculumminus) located on the anterior surface of the humerus and serves as the site of attachment of the subscapularis muscle (t.subscapularis). Intertubercular furrow (sulcusintertubercularis) located between the greater tubercle and the crest of the greater tubercle (cristatuberculimajoris) on one side and the lesser tubercle and the crest of the lesser tubercle (cristatuberculiminoris) on the other, in which the tendon of the long head of the biceps brachii passes (t.bicepsbrachii). Surgical neck (collumchirurgicum) located below the tubercles and corresponds to the location of the epiphyseal cartilage.
shoulder joint (ariiculatiohumeri) formed by the head of the humerus (caputhumeri) and articular cavity of the scapula (cavitas glenoidalis scapulae).
The size of the articular cavity is four times less than the head of the humerus, and its volume increases due to the cartilaginous articular lip (labrum glenoidale), which is also a shock absorber that softens sudden movements in the joint. However, the remaining incongruence is the cause of dislocations of the humerus.
Between the outer end of the coracoid process and the middle part of the inner surface of the acromion, a dense, 0.8-1 cm wide lig. coracoacromiale. Being above the joint, this ligament, together with the acromion and the coracoid process, forms the arch of the shoulder. The arch limits the abduction of the shoulder upward in the shoulder joint to a horizontal level. Above the hand rises already with the shoulder blade.
Joint space of the shoulder joint projected from the front to the top of the coracoid process (palpated below the outer part of the clavicle in the depth of sulcus deltopectoralis), from the outside - along the line connecting the acromial end of the clavicle with the coracoid process, from behind - under the acromion, in the interval between the acromial and spinous parts of the deltoid muscle
Projection of the joint space of the shoulder joint outside and behind
Muscles. The main role in strengthening the shoulder joint and its capsules belongs to the muscles.
Bottom from the joint without covering the capsule, there is a long head m. triceps, starting from tuberculum infraglenoidale.
Outside and above the joint is covered by the deltoid muscle, which is not directly connected to the joint capsule. The muscle consists of the posterior (spinous), starting from the scapular spine, the middle (acromial) originating from the acromion and the anterior (clavicular) parts. After the convergence of the muscle fiber, the common tendon is attached to the deltoid tuberosity of the humerus.
Under the deltoid muscle is the tendon of the long head biceps brachii, starting at tuberculum supraglenoidale and passing through the joint cavity. The tendon limits the movement of the head of the shoulder upward and anteriorly and holds the articular ends of the bones.
Then the tendon lies in the intertubercular groove, surrounded by the intertubercular synovial sheath and then connects to short head starting from the coracoid process.
Joint front covers 1) short headm.biceps 2) passing next to her m.coracobrachialis(starts from the top of the coracoid process, and is attached below the middle of the medial surface of the humerus along the crest of the lesser tubercle. F-raises the arm and leads to the midline), 3) m.subscapularis beginning in the subscapular fossa, attached to the lesser tubercle and its crest. The tendon fuses with the anterior surface of the capsule of the shoulder joint, which the muscle pulls during contraction. In cases where the tendon of the subscapularis muscle with its upper part passes into the joint cavity, the upper anterior wall of the latter is somewhat weakened. F - penetrates the shoulder and participates in bringing it to the body. Innervation n. subscapularis (C5-C7). Blood supply a. subscapularis. and also 4) the most superficially located m.pectoralismajor, which starts from the clavicle, sternum, cartilage of 2-7 ribs, attaching to the crest of the large tubercle. F- leads and rotates the shoulder inward. Innervation n. pectoralis medialis et lateralis (C5-Th 1). Blood supply a. thoracoacromialis, thoracica lateralis.
Behind and from above the shoulder joint is covered by a tendon m.supraspinatus, which begins in the supraspinous fossa, passes under the acromion, attaching to the large tubercle of the humerus. The terminal tendon fuses with the posterior surface of the articular capsule and, during its contraction, pulls it away, preventing infringement. F- abducts the shoulder, slightly turning it outward. Innervation n. Suprascapularis (C5-C6). Blood supply a. Suprascapularis, circumflexa scapula.
Behind shoulder joint is also located tendon m.infraspinatus, which starts from almost the entire surface of the infraspinatus fossa and is attached to the large tubercle of the humerus below the attachment point m. supraspinatus and above the attachment of the tendon m. teres minor. The infraspinatus muscle is fused with the capsule, covered from above by the deltoid and trapezius muscles, and in the lower sections by the latissimus dorsi and the large round muscle. F- lifts the raised arm back and rotates the shoulder outward. Innervation n. Suprascapularis (C5-C6). Blood supply a. Suprascapularis, circumflexa scapula.
Besides, behind shoulder joint covered by tendon m.teresminor starting from the lateral edge of the scapula and attached to the large tubercle of the humerus. The tendon fuses with the posterior surface of the articular capsule of the shoulder joint and, when contracted, pulls the capsule away. F- supinates the shoulder (rotates the shoulder outward) somewhat retracting it backwards. Innervation of n.axillaris (C5-C6). Blood supply a. circumflexa scapula.
Thus, from above and behind the joint capsule is strengthened by ligaments and tendons of the muscles, but from below and from the inside there is no such strengthening. This is largely responsible for the fact that in most cases the head of the humerus is dislocated forward and inward.
Articular capsule of the shoulder joint loose and relatively thin. It is attached on the shoulder blade to the bone edge of the articular cavity and, covering the head of the shoulder, ends at the anatomical neck. In this case, both tubercles remain outside the joint cavity.
Articular capsule of the shoulder joint. rear view and.
From the inside and from below, the articular capsule is attached much lower, at the level of the surgical neck of the shoulder, forming the so-called axillary torsion, recessus axillaris.
Fibrous layer of the joint capsule has thickened and weak areas. Thickened are formed due to ligaments, the most pronounced of them is lig. coracohumerale, starting from the outer edge of the coracoid process and heading to the large and, to a lesser extent, to the small tubercles of the humerus. Moreover, most of its fibers are woven into the capsule in the upper and rear parts. The ligament is located between the tendons of the supraspinatus and subscapularis muscles. Unstable occurs in 59% of cases.
Ligaments and arch of the shoulder
Little developed (better defined on the inner surface of the capsule) so-called glenohumeral ligaments, ligg. glenohumerale, or Flood's bundles[Flood], top, middle and bottom. They are stretched between the anatomical neck and labrum glenoidale. Between bundles remain weak points. The capsule is especially thin between the middle and lower ligaments - this place is the anterior "weak point" of the capsule. In the absence of the middle ligament (occurs in 1/6 of cases), a dislocation in the shoulder joint can easily be obtained.
Ligaments of Flood and intertubercular volvulus

inversions. The cavity of the shoulder joint is expanded due to three inversions(protrusions of the synovial membrane): axillary, intertubercular and subscapular. During torsions, the joint capsule is least resistant to pressure from the fluid accumulated in its cavity, and with purulent omarthritis, it is here that pus breaks into neighboring areas, forming para-articular streaks.
Axillary volvulus(recessus axillaris) corresponds to the anterior-lower section of the capsule, which is located in the gap between the subscapularis and the beginning of the long head of the triceps muscle and descends to the surgical gap of the shoulder. Immediately medially from the axillary torsion at the place of its attachment to the surgical neck, the axillary nerve passes, which, when dislocated, is often damaged and involved in the process of arthritis. Behind the axillary torsion is covered m.teres minor, which allows you to approach it through the gap between this muscle and the infraspinatus without coming into contact with the axillary nerve passing in the quadrilateral hole. Axillary torsion, being more free and low located, can serve as the main place for the accumulation of pus during inflammation of the joint. Pathways for the spread of purulent streaks from the axillary torsion down through the 3rd or 4th lateral holes into the axillary fossa or along the long head of the triceps into the posterior fascial bed of the shoulder.
Intertubercular inversion represents essentially the synovial sheath of the tendon of the long head of the biceps. It lies on the anterior-lateral surface of the proximal end of the humerus in the intertubercular groove. In this area, the articular capsule is thrown in the form of a bridge over the groove, and then only its synovial layer continues into the groove, forming a finger-like pocket surrounding the tendon of the long head of the biceps brachii, ending blindly at the level of the surgical neck of the humerus. Due to the dense covering of the intertubercular torsion by the tendons, pus rarely breaks through it. If this happens, then the pus enters the subdeltoid space and the anterior fascial bed of the shoulder with secondary streaks along the neurovascular bundles.
Subscapular volvulus located at the level of the anterior-upper section of the neck of the scapula and is a synovial bag of the subscapularis muscle, ( bursasynovialissubscapularis) located on the anterior surface of the joint capsule under the upper section of the subscapularis tendon and always communicating with the joint cavity by one or two holes. When the subscapular torsion ruptures, the pus spreads posteriorly and medially into the subscapular bone-fibrous bed or into the armpit.
Bags and twists

Synovial bags. Around the joint there is a significant number of synovial bags that make up the sliding apparatus of the muscle-tendon formations.
In addition to the already known bursasynovialissubscapularis(subscapular torsion) located on the border of the deltoid and subclavian regions, between the neck of the scapula and the tendon of the subscapularis muscle, there is also a higher and more superficial bursasubcoracoidea, located between the base of the coracoid process and the upper edge of the tendon of the subscapularis muscle. Often the sub-beak-shaped bag is also the same as the subscapularis reported with the cavity of the shoulder joint.
The location of the synovial bags of the shoulder joint. Front view

Often these two bags merge. Bursam.coracobrachialis located under the coracoid process and and the beginning m.coracobrachialis. It often communicates with the joint cavity.
On top of the large tubercle and tendon of the supraspinatus muscle lies a significant bursasubdeltoidea, which often communicates with the subacromial bursa (bursa subacromialis) lying above it. The last bag is located between the acromion and lig. Coracoacromiale. Both of these bags with the joint cavity are usually not communicated.
bursa subacromialis, bursa subdeltoidea and bursa subtendinea infraspinati
At the point of attachment of the infraspinatus muscle to the greater tubercle, there is bursasubtendineainfraspinati(sometimes communicating with the joint cavity).
Cross section at the level of the head of the humerus
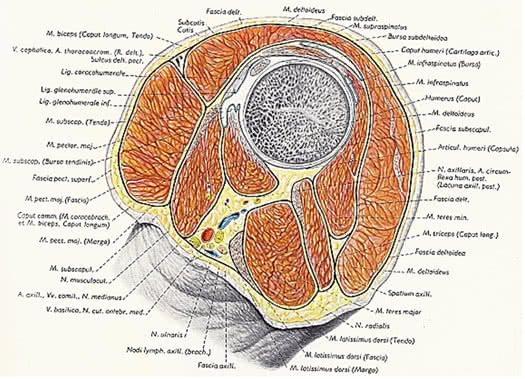
In the region of the shoulder joint, in addition to those discussed above, there are a number of synovial bags that are not associated with the joint cavity. Bursa m. latissimi dorsi subtendinea in the amount of one or two is located in the area of attachment of the muscle to the humerus on its anterior surface. At the place of attachment of the large round muscle to the crest of the small tubercle of the humerus, there is a bursa subtendinea m. teretis majoris. Between the crest of the large tubercle and the tendon of the pectoralis major muscle is located bursa subtendinea m. pectoralis majoris. There is a fickle bursa m. supraspinati.
Synovial bags of the shoulder joint
Synovial bags play an important role in the pathology of the shoulder joint and can be the beginning of the development of the inflammatory process, both in the joint and in the surrounding cellular spaces.
Permanent sources of innervation of the capsule of the shoulder joint are the axillary (C5-C6) and suprascapular nerves (C5-C6).
It is possible to damage the suprascapular nerve in case of injury with a significant displacement of the scapula laterally or dorsally.
At the same time, the tunnel syndrome of the suprascapular nerve is known, first described in 1960 by N. Kopell, W. Thompson under the name "trap" neuropathy of this nerve. In order to understand the genesis of the syndrome, it is necessary to consider some topographic and anatomical facts. The suprascapular nerve originates from the superior trunk of the brachial plexus, forming from the C5 and C6 roots. The nerve runs down behind the brachial plexus to the superior edge of the scapula. At the upper edge of the scapula, the nerve passes through the suprascapular notch, which is turned into an opening by the superior transverse ligament of the scapula. After passing through the notch, the nerve reaches the posterior surface of the scapula in the supraspinatus fossa. Here it innervates the supraspinatus muscle, gives articular branches to the shoulder and acromioclavicular joints. Then it wraps around the lateral edge of the spine of the scapula and reaches its end in the infraspinatus muscle, which it also innervates.
The passage of the nerve in the suprascapular foramen is fraught with compression during tension and bending of the nerve over the edge of the foramen. A similar condition can occur with forced, crossing the midline of the body, adductive movement of the arm. This movement causes rotation and displacement of the scapula around the back of the chest. This movement increases the tension of the nerve (the distance from the cervical origin of the nerve to the suprascapular notch increases), as a result of which the nerve is subjected to compression. As a diagnosis of the tunnel syndrome of the suprascapular nerve, the “Napoleon pose” (crossing the arms on the chest) is used. At the same time, a tensely straightened arm passively moves to the other half of the body with the intersection of its midline. With this movement, the displacement of the scapula causes extremely pronounced pain as a result of tension and pinching of the nerve.
The suprascapular nerve has no cutaneous sensory branches, but carries propriosensitivity from innervated muscles and joints. Therefore, when the nerve is compressed, the pain is characterized as deep, "tedious", aching, with localization in the area of the scapula along the back and outer surface of the shoulder.
In the diagnosis of the tunnel syndrome of the suprascapular nerve, the appearance of pain on palpation of the projection site of the suprascapular nerve at the entrance to the notch of the scapula is also used.
Damage to the axillary nerve can occur when the shoulder is dislocated, with strong traction on the arm to eliminate the dislocation, ( one in 7 dislocations of the shoulder is complicated by nerve palsy due to primary stretching of the branches of the brachial plexus) much less often as an isolated injury. It is manifested by paresis or paralysis of the deltoid muscle, the absence of active shoulder abduction, loss of skin sensitivity in the deltoid region and along the anterior surface of the shoulder. Clinically and radiologically, a downward displacement of the head of the humerus is determined, which stimulates subluxation or dislocation of the shoulder.
The location of the axillary nerve next to the axillary volvulus does not exclude the transition of inflammation to the nerve in omarthritis.
The passage of the axillary nerve in the quadrilateral hole causes the possibility of compression of this nerve, because. this hole narrows significantly with simultaneous abduction and flexion of the shoulder. Cases of compression of the axillary nerve in dentists are described, often forced to carry out professional movement (abduction and simultaneous flexion of the shoulder), which led to re-traumatization of the nerve (Zhulev N.M. et al., 1992)
Blood supply aa. circumflexae humeri anterior et posterior and additionally through deltoid and acromial branches from a. thoracoacromialis.
Sometimes the displaced head of the shoulder presses on the vessels in the armpit. Until the dislocation is reduced, the hand may remain cyanotic and cold. In rare cases, there is a rupture of the axillary artery and the formation of a traumatic aneurysm, especially when trying to reduce the old dislocation by violent manipulations.
SOME ASPECTS OF THE TOPOGRAPHIC ANATOMY OF THE SHOULDER JOINT MUSCLES
In the region of the shoulder joint there are various anatomical formations (bones, cartilages, muscles, synovial bags, vessels, nerves, etc.) pathological changes in which can manifest themselves with a variety of clinical symptoms, and it is necessary to begin to understand its nature with a clear understanding of the structure, relative position and the functions of these anatomical structures.
The purpose of this short review is to consider some topographic and anatomical features of the structure of the muscle layer of the shoulder joint area.
The pathology of the muscles located in the area of the shoulder joint causes limitation of mobility in it and the appearance of pain in the areas adjacent to the joint. The cause of muscle pathology, first of all, is an acute or chronic injury that can lead to tendon rupture, or to the development of degenerative changes in muscle, tendon tissue, or even in the joint capsule. The appearance in the muscle of an isolated focus of tension and pain is accompanied by irradiation of pain in the adjacent anatomical regions. These states are described under different names (muscular rheumatism, myofascial syndrome, myofasciitis and etc.). Lesions of individual muscles located near the shoulder joint have received a variety of names (frozen shoulder, silver dollar pain symptom, shoulder pain symptom, subdeltoid bursitis mimic and etc.).
The shoulder joint has a much wider range of motion than any other joint. The extensible capsule and small, flat articular surface allow for such mobility.
Movement in the shoulder joint is carried out around three main axes: around the frontal - flexion (movement of the upper limb forward and upward) and extension (movement of the limb back and upward); around the sagittal - abduction (movement of the limb to the side and up) and adduction (movement of the limb down to the body); around the vertical axis - rotation of the lowered limb with the palm inward (pronation) and rotation with the palm outward (supination). In the joint, circular motion (circumduction) is also possible - movement alternately around many axes, when the entire limb describes the shape of a cone. According to V. A. Gamburtsev (1973), the amplitude (span) of movements in the shoulder joint normally at the age of 10 to 40 years varies within the following limits (initial position - the limb is lowered along the body): flexion - 181-179 °; extension - 89-85 °; – 184-179°; pronation - 103-102 °; supination - 45-42 °. Moreover, flexion and abduction above the horizontal position of the limb occur in combination with the movement of the shoulder girdle.
Muscles (supraspinatus, infraspinatus, teres minor and subscapularis) that rotate the shoulder formROTATOR CUFF (BasmajianJ. V . 1978). All these muscles, starting on the scapula, are attached to the large and small tubercles of the humerus.
The tendons of the muscles of the supraspinatus, infraspinatus and subscapularis on each side form a thick continuous layer, soldered to the underlying articular capsule and separated from the deltoid muscle and the acromial process by a mucous bag.
An important function of the rotator cuff muscles is to stabilizeheads of the humerus in the glenoid fossa during hand movements. With the pathology of the muscles that make up the rotator cuff, decentralization of the head can occur, resulting in pain and impaired movement in the shoulder joint.
In this regard, we will consider some of the practical topographic and anatomical features of the structure of each of the muscles that make up the rotator cuff.

supraspinatus muscle the medial end is attached to the supraspinous fossa of the scapula, and the lateral end, passing under the acromion, to the upper part of the large tubercle of the humerus.

Knowing the points of attachment and the course of the supraspinatus muscle helps to understand its function, the idea of which allows you to better understand some of the points associated with the pathology of this muscle. The supraspinatus muscle abducts the shoulder and pulls the head of the humerus medially into the glenoid cavity, which prevents the head from moving down when the arm is freely lowered. Based on this, the mechanism becomes clear pathognomonic for a complete rupture of the tendon of the supraspinatus muscle symptom of "falling hand". The hand, passively raised to a vertical position, falls when you try to lower it, i.e. the patient cannot actively hold it in the abduction position. With a complete rupture of the tendon of the supraspinatus muscle, the deltoid muscle alone cannot fully abduct the shoulder and in such patients it becomesit is possible to actively abduct the arm only up to 60 ° due to the movement of the scapula.
The fact that the main function of the supraspinatus muscle is shoulder abduction makes clear the genesis of the main complaint of patients with the pathology of this muscle for pain, which increases withmovement of the limb to the side and up. And at rest, which is typical, the pain is not intense and is dull in nature.
A violation of shoulder abduction explains the difficulties that arise when the supraspinatus muscle is damaged, the difficulties experienced by patients when raising their hands to their heads in order to comb their hair, brush their teeth, etc.
When the supraspinatus muscle is damaged, the tension of its fibers appears, which disrupts the normal sliding of the head of the humerus in the glenoid fossa. Apparently, this explains the crunch or clicking in the area of the shoulder joint that occurs in some patients with pathology of the supraspinatus muscle, disappearing after the elimination of muscle tension.
Features of the topographic anatomical location of the muscle cause the appearance of pain in the pathology of the supraspinatus muscle in the shoulder girdle. Pain is especially pronounced in the middle of the deltoid region. And this localization of pain, given the location above the tendon of the supraspinatus muscle and greater tubercle of the humerus bursasubdeltoidea ( the size of the bag corresponds approximately to the palm of the patient) is often mistakenly perceived as a symptom of subdeltoid bursitis (subdeltoid bursitis simulator) In these cases, as one of the methods of differential diagnosis, the determination of point pain in the area of the supraspinatus muscle can help. After finding such points of palpation soreness, local anesthetics are injected into them for diagnostic and therapeutic purposes. Taking into account that the supraspinatus muscle is innervated by the suprascapular nerve, it is proposed ( SkillernP. G .), in order to relieve pain in the shoulder girdle that did not find an explanation, accompanied by soreness on palpation of the supraspinatus muscle, to blockade the suprascapular nerve.
The location of bursasubdeltoidea, bursasubacromialis relative to m. supraspinatus and acromion
Above the subdeltoid bag is located between the acromion and lig. coracoacromiale subacromial bag. Most often, these bags communicate with each other. Each abduction of the shoulder between 60° and 120° creates friction between the supraspinatus tendon and the acromial process, which is reduced by the presence of a mucosal sac that lies between them.
Contact m. supraspinatussacromione during arm abduction


Over time, especially in people engaged in heavy physical labor associated with strenuous shoulder movements, the walls of the bag are damaged, and it ceases to serve as sufficient protection. Constant re-traumatization causes degenerative changes in the tendons and joint capsule. Such degenerative changes predispose to supraspinatus tendon calcification. Such deposits increase the pressure on the acromial process, which makes the pain much worse than with simple inflammation of the tendon sheaths. Abraded necrotic fibers are extremely sensitive to any damage and a simple fall or sudden muscle tension can cause an incomplete or even complete rupture of the tendons. Degenerative changes can spread to the adjacent long head of the biceps muscle, which spontaneously ruptures, or to the entire tissue of the capsule, causing periarthritis and the formation of periarticular adhesions. One of the symptoms of inflammation of the tendon of the supraspinatus muscle may be pain when the shoulder is abducted in the range from 60 to 120 °, i.e., in the range when the tendon is clamped by the edge of the acromial process. Beyond this, when the limb is in full abduction, the movements cease to be painful, as the sensitive area is protected by the acromial process, not in contact with it. Likewise, as the shoulder descends, there is sharp tenderness again between 120° and 60° abduction. This symptom can be differentially significant, since in arthritis of the shoulder joint, pain appears immediately with the onset of movement and continues with the entire range of movements. With adhesions in the area of the shoulder joint, pain occurs when the shoulder is abducted by 70-80 °, but continues with further abduction.
infraspinatus muscle Of particular importance for differential diagnosis in rheumatology are information about the pathology of the infraspinatus muscle. Many authors point out that pain emanating from the infraspinatus muscle very accurately imitates pain that occurs in the shoulder joint itself (symptom of shoulder pain, and can be mistaken for symptoms of arthritis of the shoulder joint. When the infraspinatus is affected, the main localization of pain is the anterior region of the shoulder joint, but the pain can also be projected down into the anterior-lateral region of the shoulder. This nature of pain requires finding out the location of the muscle.
The infraspinatus muscle starts from more than 2/3 of the surface of the infraspinatus fossa of the scapula and goes laterally and is attached to the posterior surface of the large tubercle of the humerus.

Muscle covered from above by the deltoid and trapezius muscles, and in the lower sections by the latissimus dorsi and the large round. Blood supply a. Suprascapularis, circumflexascapula . With pain in the shoulder joint caused by the pathology of the infraspinatus muscle, it is possible to determine the zones of local pain in the muscle itself using deep palpation. Most often, pain is detected at a point below the lateral border of the medial 1/3 of the scapular spine and equidistant from the spine and the medial angle of the scapula, or in the area below the middle of the scapular spine. In addition, in the area of the affected subscapularis muscle, sometimes tight bands are palpated.
The muscle is innervated n. suprascapularis , departing through the upper trunk from the 5th and 6th cervical nerves. Infraspinatus pathology causes pain in areas innervated by the 5th, 6th, and 7th cervical nerves, which can lead to a misdiagnosis of radiculopathy due to intervertebral disc disease ( ReynoldsM. D. 1981)
The infraspinatus muscle rotates the shoulder outward in any position and is involved in stabilizing the head of the humerus in the glenoid cavity when the arm is raised up. In addition, the upper muscle fibers are involved in abduction (raised hand is pulled back), and the lower ones in adduction of the shoulder. The infraspinatus muscle, together with the small round muscle and the posterior fibers of the deltoid muscle, rotates the shoulder outward. The infraspinatus muscle helps the supraspinatus and other rotators of the shoulder stabilize the head of the humerus in the glenoid cavity during abduction and extension of the shoulder.
Interesting from our point of view is the fact that in the case of reflection of myofascial pain in the shoulder joint, the source of this pain, according to a number of authors, is most often localized in the infraspinatus or supraspinatus muscles. Perhaps this is due to the common innervation of these muscles by the suprascapular nerve. It is unlikely that such localization of pain is a direct consequence of the contractile activity of these muscles. After all, the infraspinatus and supraspinatus muscles have different functions, but at the same time cause deep pain in the area of the shoulder joint, at the same time, the infraspinatus and small round muscles perform almost the same actions, but have different innervation and different localization of pain.
Information about the function of the muscle helps to explain the reason for the appearance of patients' complaints that they cannot reach the back pocket of their trousers with their hand, cannot fasten their bra, etc. When performing these movements, it is required to turn the shoulder inward, which should be accompanied by stretching of the muscles that rotate the shoulder outward. And with damage to the infraspinatus muscle, leading to tension and shortening of muscle fibers, the patient is not able to reach even the back pocket of his trousers with his fingers. Moreover, the restriction of this movement is the same for both active and passive execution.
TERMINAL MUSCLE starts from the posterior surface of the lateral edge of the scapula and is attached to the lower facet of the large tubercle of the humerus below the tendon of the infraspinatus muscle. The tendon fuses with the posterior surface of the articular capsule of the shoulder joint and, when contracted, pulls the capsule away. Blood supply a. circumflex capula. Innervation n. axillaris (C 5-C 6).
An isolated lesion of the teres minor muscle has been described in the literature as pain zone symptom the size of a silver dollar . This is caused by patients complaining of pain in an area the size of a silver dollar (diameter of an American silver dollar is 32 mm) deep in the back of the deltoid muscle just proximal to its attachment to the deltoid tuberosity of the humerus. Perhaps the localization of pain in the deltoid region is somehow connected with the fact that the small round and deltoid muscles are innervated by the same nerve. The pain is perceived by the patient as deep and well-defined and may be misinterpreted as bursitis. To make a correct diagnosis, one should take into account the pathognomonic localization of pain in the area located significantly below the subacromial sac.
The small round muscle supinates the shoulder (rotates the shoulder outward) somewhat retracting it posteriorly. Many authors identify the actions of the small round and infraspinatus muscles. Both muscles rotate the shoulder outward regardless of the position of the arm (abducted, bent, straightened) and are involved in stabilizing the head of the humerus in the glenoid cavity during arm movements.
Stroke and topography and m . teresminor


Myofascial teres minor syndrome is uncommon ( SolaA . E ). Even more rare is an isolated lesion of the small round muscle. As a rule, there is a combined pathology of the small round and infraspinatus muscles. Moreover, the pain from the latter is clearly dominant, and the elimination of tension of the infraspinatus muscle contributes to the detection of pain irradiation from the small round muscle. Probably, this combination of pathology can be explained by the fact that the small round muscle, according to the figurative expression of D.G. Trevella, functions as a younger brother in parallel with the infraspinatus muscle. These muscles have adjacent areas of anatomic origin and attachment, but different innervation. The same role of the “younger brother” can probably explain the fact that with an isolated lesion of the small round muscle, patients complain more about pain than about limited movement. Probably, there is a compensation of movements due to the infraspinatus muscle.
SUBSHELLAR MUSCLE starts from the anterior surface of the scapula, filling the subscapular fossa from the medial to the lateral edge. Heading laterally, it passes into the tendon, which crosses the shoulder joint in front and is attached to the lesser tubercle of the humerus and to the lower anterior part of the articular capsule of the shoulder joint. Cases are described when the tendon with its upper part passes through the cavity joint, as a result the upper anterior wall of the latter is somewhat weakened. The subscapularis muscle is attached to the humerus most anteriorly of all the other muscles that form the rotator cuff (infraspinatus, supraspinatus and small round muscles).
The site of the shoulder attachment of the subscapularis is usually very painful in the chronic nature of myofasciitis. To examine the shoulder attachment of the muscle, the patient brings the shoulder to the body, trying to reach the back with the elbow, turns the shoulder outward. With this movement of the shoulder, the area of attachment of the subscapularis muscle to the humerus comes out from under the humeral process forward and becomes available for palpation. The synovial subscapular bag, which communicates with the cavity of the shoulder joint, separates the neck of the scapula from the subscapularis muscle. Innervation n. subscapularis (C 5-C 7). blood supply a. subscapularis.
Stroke and topography m . subscapularis
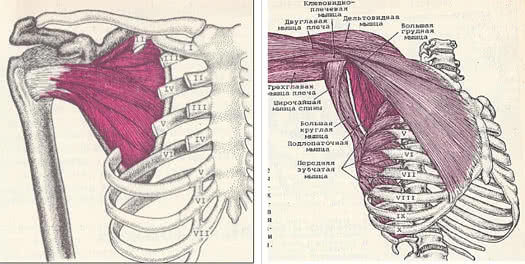
The subscapularis muscle rotates the shoulder inward (pronates) and brings it to the body, and together with other muscles holds the head of the humerus in the articular cavity. shoulder process, however, the subscapularis muscle counteracts this displacement of the head.
The concept of the nature of the actions of the subscapularis muscle will help to understand the mechanism of dysfunction of the hand that occurs in the pathology of the subscapularis muscle. The pathological process in the subscapularis muscle can lead to a strong shortening of this muscle, as a result of which the muscle holds the shoulder in an inwardly turned position and the person cannot fully supinate the hand with a straightened arm due to the limited outward rotation of the shoulder.
The defeat of the subscapularis muscle causes severe pain, both at rest and during movement. The main pain zone is located in the area of the posterior projection of the shoulder joint, but can spread down the back of the shoulder to the elbow. In some patients, there is referred pain and tenderness in the form of a cuff encircling the wrist, which is of diagnostic value, and on the back of the wrist, pain and tenderness are more pronounced than on its palmar side. Because of pain in the wrist, patients put the watch on the other hand. In the early stages of subscapularis involvement, patients can lift their arm up and forward, but they cannot swing their arm back when, for example, they are trying to throw a ball. According to TravellJ . G ., the appearance of a focus of tension in the subscapularis muscle leads to a gradual increase in the limitation of mobility in the joint due to pain, which causes damage to the large and small pectoral, large round, latissimus dorsi, triceps and, finally, the deltoid muscles. Eventually, all muscles can be affected shoulder girdle. From this point on, none of the affected muscles can be stretched to its full length, all movements in the shoulder joint are severely limited. The shoulder joint becomes "frozen" , and trophic disorders often follow. However, it should be noted that the term “frozen shoulder” is interpreted differently in the literature, numerous reasons for the development of limitation of movement in the shoulder joint are given, and various clinical symptoms of this disease are given.
Knowledge of the topographic anatomy of the subscapularis muscle gives an understanding that an isolated lesion of this muscle limits mobility in the shoulder joint, but does not impair the movement of the scapula relative to the chest. Therefore, when examining a patient who has limited shoulder movement, the first thing to check is the mobility of the scapula. To this end, the doctor puts his hand on the patient's shoulder blade and invites him to take his hand away. If, in addition to limiting mobility in the shoulder joint, the mobility of the scapula is limited, then the pathology of the pectoralis minor, anterior dentate, trapezius and rhomboid muscles should also be suspected.
IMPIGEMENT SYNDROME. When the arm is raised, even in normal conditions, there is a slight compression of the tendons between the head of the humerus and the acromion.
In the case of a narrowing of the gap between the acromion and the tendons of the rotator cuff, impingement syndrome occurs, which consists in injuring the muscles of the rotator cuff. In the early stages of the development of impingement syndrome, the main complaint of patients is diffuse dull pain in the shoulder. The pain is aggravated by raising the arm up. Many patients report that pain prevents them from falling asleep, especially when lying on the side of the affected shoulder joint.
The pathognomonic symptom of impingement syndrome is the occurrence of acute pain in a patient when trying to reach the back pocket of his trousers or unbutton his bra. In later stages, the pain intensifies, possibly the appearance of joint stiffness.
Sometimes there is a clicking in the joint when the arm is lowered. Weakness and difficulty in raising the arm up may indicate a rupture of the rotator cuff tendons.
The relationship of the acromion and the muscles of the rotator cuff when the arm is raised
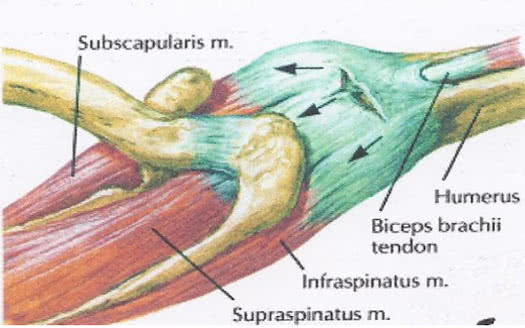
Thus, the clinic of impingement syndrome consists of manifestations inherent in damage to the muscles that make up the rotator cuff.
We also recommend
 Enchantment teachers in Skyrim: what do they give, where to find?
Enchantment teachers in Skyrim: what do they give, where to find?
 Changing the appearance of characters with Face Ripper and Fo4edit
Changing the appearance of characters with Face Ripper and Fo4edit
 Download sandbox games torrent Skyrim mods 18
Download sandbox games torrent Skyrim mods 18
 Location of rare resources in Assassin's Creed: Syndicate Assassin's Creed Syndicate all costumes
Location of rare resources in Assassin's Creed: Syndicate Assassin's Creed Syndicate all costumes
 Skyrim crashes when saving
Skyrim crashes when saving
 A night to remember (Sanguine)
A night to remember (Sanguine)